|
(Print this page, complete & mail to ACA)
Name (please print)____________________________________ Referred by : Frank A. Stiso,D.C.
Address:_______________________________________________________________________________
Office Phone(_____)_____________________ Home Phone(_____)_____________________ Fax(_____)______________________
E-Mail______________________
Chiropractic College _______________________Degree_______ Date of Graduation__________
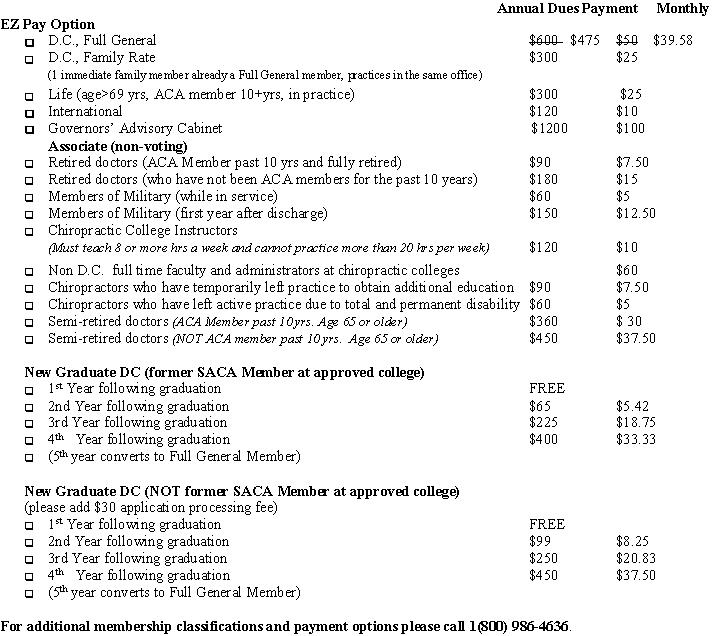
*This is a one-time offer to join/rejoin the ACA for a reduced payment of $475 for the first year of D.C Full General dues.
This offer is for a limited time only and cannot be combined with any other special offer to join the ACA. Annual dues payment
or enrollment in EZ Pay must accompany this completed membership application to validate this offer. Membership application
is subject to review and approval by ACA's Membership Committee. Valid only to those who have not been ACA members for at
least 12 months. Annual dues include $90.00 for a subscription to the Journal of American Chiropractic Association. In 2003,
Ninety-three percent of ACA membership dues may be deductible as an ordinary and necessary business expense. In applying
for membership, I certify that I am registered and/or licensed. I understand that my application is subject to ACA Board
approval, that will I will be notified of its action, that failure to remit will result in loss of membership, and that membership
includes all rights and privileges as provided in ACA Bylaws. I pledge to ascribe to ACA's profound commitment to top quality
care, professionalism, and ethics. I respect the unique individuality of my patients and am dedicated to protecting and preserving
their rights.
Applicant Signature:______________________________ Date:_________
1701 Clarendon Blvd Arlington VA 22209 * 703/276-8800 * Fax 703/243-2593 * memberinfo@amerchiro.org * www.acatoday.com
Mail or Fax to: The American Chiropractic Association, 1701 Clarendon Blvd, Arlington, VA 22209.
Fax (703)243-2593
|
